
Urinary tract infection (UTI)
About 20 percent of all women have urinary tract
infections (UTI) during their lifetime. The cases are
often overlooked or ignored when the manifestations
are minor. Moreover, in cases of asymptomatic
bacteriuria, the infection remains in the urinary tract

Male and female reproductive system
for a long period of time only to flare up to produce
pyelonephritis in significant cases. As such, due
attention should be paid even in asymptomatic patients
having significant bacteriuria.
Organisms :
The commonest organism is Escherichia
coli which is present in about 80–90 percent cases. Others
are Pseudomonas, Klebsiella, Proteus, Enterococci,
Staphylococcus, etc.
Causes of urinary tract infection:
� The lower urethra is colonized with bacteria
early in life but the bacteria are non-pathogenic.
The protective effect of estrogen is also lacking.
� Sexual intercourse increases the ascent of the
organisms from the lower urethra into the bladder.
� Full bladder—Provided bladder is kept empty
completely and regularly, there is least chance of
UTI. But certain circumstances favor atonicity
of the bladder and urinary stasis as in pregnancy,
puerperium and following major pelvic surgery or
pelvic tumors producing outflow tract obstruction.
� Catheterization—This is probably the commo-
nest cause of introducing the organisms from
the lower urethra into the bladder whatever
meticulous aseptic technique being taken. It has
been observed that an indwelling catheter kept for
24 hours will produce bacteriuria in 50 percent
and if left for 4 days will lead to bacteriuria in 100
percent of cases.
� Hypoestrogenic state as in postmenopausal
women—when defence of the bladder and urethral
mucosa is diminished.
� Immunocompromising disorders like diabetes
mellitus, HIV.
Route of infection
• Ascending
• Hematogenous
• Lymphatic
Ascending—is the commonest route of infection.
The organisms from the anorectal region, lower vagina
and vulva gain access to the urethra and thence to the
bladder and kidneys.
Hematogenous—spread involving the kidneys is
from the intestine or septic tonsils or other septic foci.
Lymphatic—spread is either from the adjacent
ascending colon or genital organs (cervicitis). The
kidneys may be affected from the bladder through
periureteral lymphatics.
Clinical presentation :
Lower urinary tract infection
Urethritis: The symptoms include dysuria,
frequency and urgency of micturition. Pain is typically
scalding during the act of micturition. Urethra is
tender on palpation. Often, pus may be squeezed out
from the urethra.
Apart from clean catch midstream urine for culture,
the expressed pus should be submitted for Gram stain
for intracellular diplococci suggestive of gonorrhea
and culture for Chlamydia and Neisseria gonorrhoeae.

Sign and symptoms of UTI
Urethral syndrome: It is a chronic non-
specific form of urethritis probably due to urethral
hypersensitivity. Infection should be excluded. The
symptoms include dysuria, frequency, nocturia
and urgency of micturition. Urethroscopy reveals
reddened, chronically inflamed urethral mucosa
and spasm of the bladder-neck. Benzodiazepines,
Amitriptyline. Antibiotics (doxycycline) and estrogen
replacement therapy give short-term relief. Progressive
urethral dilatation has been the treatment of choice.
Cryosurgery has been found to be effective to relief
the symptoms.
Cystitis:Cystitis is the most common of the urinary
tract infections.
Symptoms include dysuria, frequency and urgency
of micturition and pain. It produces painful micturition
especially at the end of the act. There may be
suprapubic tenderness and may have constitutional
upset.
Investigations: Midstream clean catch urine for
microscopic examination, culture and drug sensitivity
is to be done in every case.
Microscopic examination usually reveals plenty of
pus cells and occasional red blood cells. The culture
will detect the organism within 24 hours and it usually
exceeds 105
/mL of urine.
Sterile pyuria (negative culture in presence of
plenty of pus cells) alerts the possibility of tubercular
infection. In suspected tuberculosis, at least three
early morning urine specimens have to be collected
and cultured.
The presence of red blood cells in the absence
of pus cells or negative culture suggests pathology
other than infection.
Apart from midstream urine, other methods of
collection of urine are—suprapubic needle aspiration
and urethral catheterization.
Pyelitis: Symptoms include acute aching pain over
the loins and fever with chills and rigor. There is
frequency of micturition and dysuria. There may be
anorexia, nausea or vomiting.

Prevention
� To maintain proper perineal hygiene. This
consists of cleansing the vulvar region at least
daily, wiping the rectum away from the urethra.
� Prophylaxis of the coital infection—To void
urine immediately following coitus. A single
dose of nitrofurantoin 50 mg following coital
act is an effective means of prophylaxis. This is
helpful in women who have history of postcoital
exacerbation of infection.
� Catheter infection—Whatever aseptic measures are
taken, use of catheter favors introduction of infection
Catheter should preferably be avoided.
� Bacteriological monitoring of urine should be
done, periodically and after removal, when an
indwelling catheter is used for a long time
� Plenty of fluid intake should be encouraged.
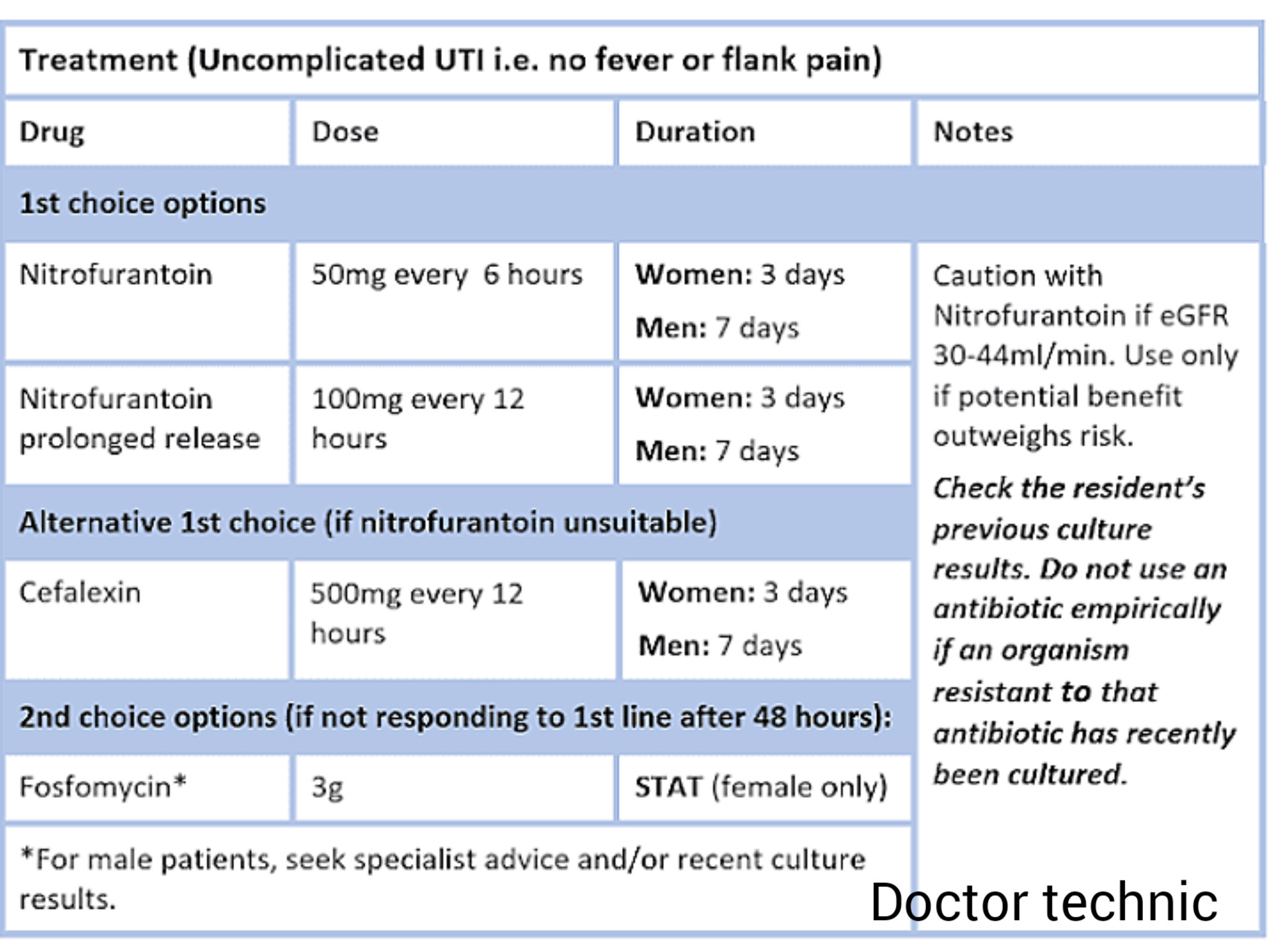
Treatment of urinary tract infection:
General measures:Plenty of water to drink (3–4
liters a day) for proper hydration.
Antimicrobial agents: Appropriate antibiotic to
be started for an adequate length of time (7–10 days).
One negative culture two weeks after the course of
therapy is considered cure.
Prevention of reinfection: Presence of any
organic pathology is to be treated. Outflow tract
obstruction, if present, may have to be dilated.
In reinfection, the appropriate drug is to be
continued for at least 2 weeks. This is to be followed
by nitrofurantoin 50 mg or norfloxacin 400 mg daily
for 4–6 months.
.png)



.png)






{kind=link}
0 Comments